Article Text

Abstract
Introduction To examine the interactions between short maternal stature, body mass index (BMI) and gestational weight gain (GWG) among appropriate for gestational age (AGA) term newborns in a population of refugees and migrants in Southeast Asia.
Methods This is a retrospective cohort study from 2004 to 2016, including women delivering term, singleton newborns, with first trimester height, weight and gestation dated by ultrasound and a last body weight measured within 4 weeks of birth. AGA newborns were those not classified as small for gestational age or large for gestational age by either INTERGROWTH-21st or Gestation Related Optimal Weight standards. The influence of maternal stature on GWG in delivering an AGA newborn was analysed, with GWG compared with existing National Academy of Medicine (NAM) recommendations.
Results 4340 women delivered AGA newborns. Mean maternal height (SD) was 151.5 cm (5.13), with 58.5% of women considered too short by INTERGROWTH-21st standards. Only one in four women (26.5%, 1150/4340) had GWG within NAM recommendations. Women of shorter stature had a significantly lower mean GWG compared with taller women in underweight and normal BMI categories (p<0.001 for both BMI categories). Mean GWG of overweight and obese women did not differ by height (p=1.0 and p=0.85, respectively) and fell within the lower range of NAM recommendations.
Conclusion These results suggest that short maternal stature can be an important predictor of GWG and should be considered with prepregnancy BMI. Limited-resource settings and special populations need robust GWG recommendations that reflect height and BMI.
- child health
- maternal health
- nutrition
- cohort study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Maternal short stature is common in low-income and middle-income countries, but the extent to which it affects gestational weight gain (GWG) and in turn, giving birth to appropriate for gestational age newborns, is unknown.
What are the new findings?
In a Southeast Asian population with a high prevalence of short maternal stature, nearly 80% of women birthed appropriate for gestational age newborns in spite of being considered ‘unhealthy’ by international standards.
Women of shorter stature had a significantly lower mean GWG compared with taller women in underweight and normal body mass index (BMI) categories.
Two-thirds of the women birthing appropriate for gestational age newborns had suboptimal GWG according to international recommendations.
What do the new findings imply?
Short maternal stature can be an important predictor of GWG and should be considered with prepregnancy BMI.
Larger data sets are needed to inform standards and data pooling should be encouraged.
Introduction
A meta-analysis in 2015 estimated that 5.5 million or 18.6% of term, small for gestational age (SGA) births are associated with short maternal stature (<155 cm). Nearly 70% of Southeast Asian women studied were of short stature.1 However, the most commonly followed guidelines for optimal gestational weight gain (GWG) to achieve appropriate for gestational age (AGA) newborns recommends GWG ranges based on prepregnancy body mass index (BMI) alone, without accounting for maternal height.2 3 The National Academy of Medicine (NAM) in the USA, which produced these guidelines, recognised their GWG recommendations may be limited in ‘special populations’ with short stature.2 Prepregnancy BMI in Asian populations may also require caution, as the WHO advises different categories for Asian populations to adjust for their risk of non-communicable diet-related disease at lower BMI.4–10 Hence, it remains unclear what recommendations address maternal stature, BMI and GWG to deliver AGA term newborns in Asian populations where short maternal stature is the norm.
Identifying AGA term newborns, however, may be easier. Two international standards for identifying SGA and large for gestational age (LGA) newborns include the population-based INTERGROWTH-21st (IG-21) Project11 and the Gestation Related Optimal Weight (GROW) customised centiles.12 IG-21 standards arose from prospective cohorts of ‘healthy’ women across eight countries, representative of multiple ethnicities.13 14 GROW standards employ ‘customised’ growth trajectories gathered from large birthweight databases and adjusts for physiologic variation with respect to ethnicity, maternal height, and parity.15 Although neither are perfect when applied to general obstetric populations,16 17 we assume that when taken together these standards can accurately identify true AGA newborns.
Marginalised populations of refugees and migrants on the Myanmar-Thailand border have emerged in the past few decades, where compromised nutrition is commonplace,18 19 and the average maternal height of 151 cm20 is on par with the shortest 3 of 132 countries.21 However, short maternal stature alone should not preclude women from being considered ‘healthy’, having healthy pregnancies, or from having realistic GWG recommendations. With well-characterised pregnancies, including height from this at-risk population and global standards to identify AGA newborns, we compared GWG for AGA newborns in this population with NAM GWG recommendations.
Methods
Setting
This retrospective cohort study collated data from refugee and migrant communities along the Myanmar-Thailand border from 2004 to 2016. Data on refugees came from Mae La camp, with an estimated 37 786 refugees in 2016.22 The Shoklo Malaria Research Unit (SMRU) provided antenatal care (ANC) services to approximately 90% of the women in the Mae La camp with 75% of them delivering at the SMRU clinic.23–25 SMRU also serves the migrant communities within Tak province, Thailand and Karen State, Myanmar, through clinics in Maw Ker Thai and Wang Pha, Thailand. The estimated catchment of these clinics is approximately 200 000 migrants.26 The predominant ethnic group along the border remains the Karen, but the flow of migrants from neighbouring Myanmar has led to a greater diversity of communities served by SMRU. Both refugee and migrant communities come from socially and economically disadvantaged situations, often from regions in Myanmar with poor access to maternal health services.27–29
Study design and participant Inclusion/exclusion
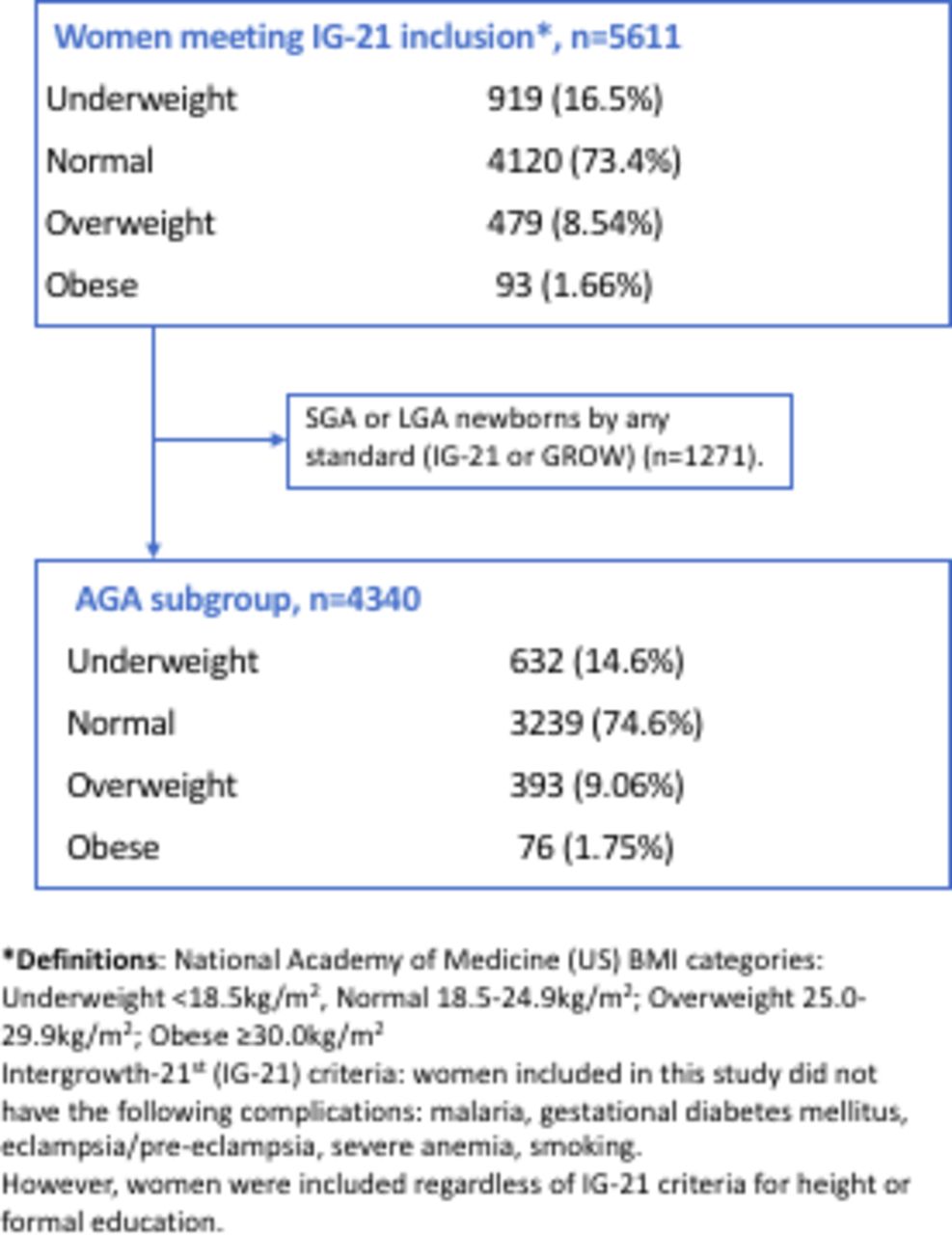
We performed a retrospective analysis of digital clinical records containing antenatal and birth details of patients receiving care at SMRU clinics from January 2004 through December 2016 (figure 1). We included only those women with a first trimester weight and height measurement as this is considered an accurate proxy for prepregnancy BMI calculations.30 Women with term (estimated gestational age (EGA) 37.0–42.0 weeks), singleton births and at least two weight measurements over the course of their pregnancy, with the last one between 34.0 and 40.0 weeks, were included. Stillbirths, early neonatal deaths in the first 7 days of life, congenital abnormalities and newborns with no birth weight measured in the first 72 hours of life were excluded.
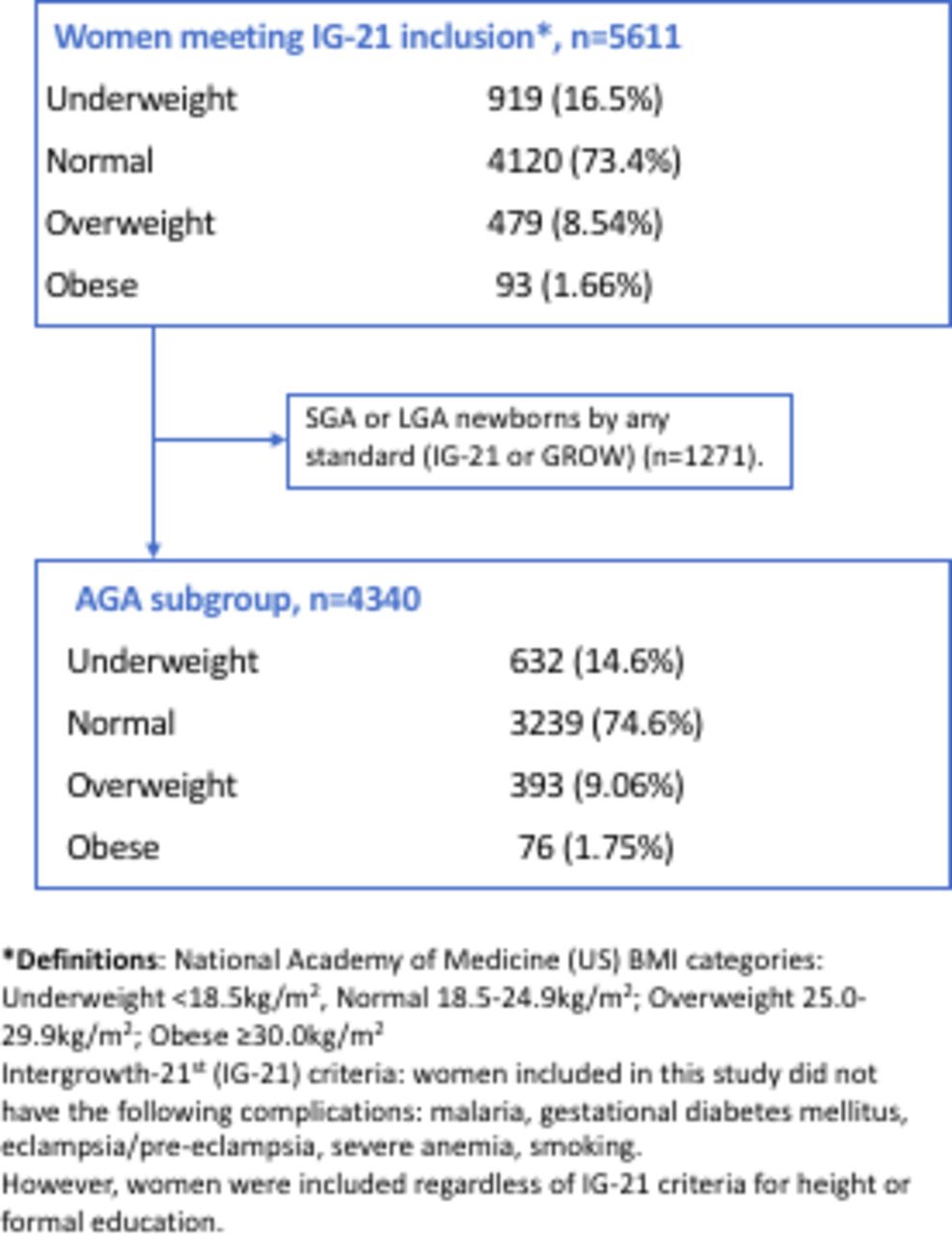
Flow of study participants: singleton pregnancies from 2004 to 2016, presenting in the first trimester, with known outcome and no pregnancy complications (IG-21st inclusion/exclusion criteria)31 and with AGA newborns (n=4340). AGA, appropriate for gestational age; BMI, body mass index; GROW, Gestation Related Optimal Weight; SGA, small for gestational age.
To facilitate comparison of this population with others in the published literature, GWG was analysed for women defined using IG-21 inclusion criteria.31 Inclusion criteria were: non-smoking, no severe medical conditions (malaria, severe anaemia, pre-eclampsia or eclampsia, postpartum haemorrhage or gestational diabetes mellitus) and age 18–35 years old (figure 1). However, to avoid excluding most women from this study population, we did not use the IG-21 exclusion criteria for maternal stature (<153 cm) or formal education.31 As we wanted analysis of GWG by BMI category, we kept in women from all BMI categories, as categorised by NAM and used by IG-21 (underweight <18.5 kg/m2, normal 18.5–24.9 kg/m2; overweight 25.0–29.9 kg/m2; obese ≥30.0 kg/m2).
Variables and measurements
Demographic variables
Information on refugee/migrant status, ethnicity (self-identified), age and parity were collected.
Anthropometric variables
Trained midwives collected weight measurements at first ANC consultation and at each follow-up visit by mechanical Salter scales with 0.5 kg precision. Midwives collected height measurements at first ANC using a mechanical stadiometer with 5 mm precision until 2010 when these were replaced with electronic stadiometers with 1 mm precision.
Estimating gestational age
EGA was calculated by ultrasound, using crown-rump length at 9+0 to 13+6 weeks according to international standards.32 The quality of ultrasound in this setting has been assessed previously and quality control of gestational age measurements is conducted twice annually.33
SGA and LGA calculations
Sex-adjusted birthweight centiles were calculated using IG-21 standards from the Fetal Growth Longitudinal Study and Newborn Cross-Sectional Study13 and using the GROW customised centile calculator V.8.0.12 15 Newborns not determined to be SGA or LGA by either IG-21 or GROW standards were assumed AGA.
Gestational weight gain
GWG was the difference between the first weight measured (in the first trimester) and the last weight measured no more than 4 weeks prior to delivery.
Analysis
Maternal demographic and birth outcomes, including IG-21 and GROW defined SGA (<10th centile) and LGA (>90th centile), were described according to BMI categories. Comparisons across BMI categories, including for GWG for delivery of AGA newborns, were made using a nonparametric test for trend across ordered groups. GWGs were compared against those recommended by NAM for each BMI category. Mean GWG according to BMI category was analysed for height categorised as <145 cm, 145–149.9 cm, 150–154.9 cm and ≥155 cm.
Data were analysed using STATA, V.15.1 (StataCorp).
Patient and public involvement in research
At the outset of the study, the research team engaged the local population through a local ethics and research advisory committee, the Tak Province Community Advisory Board, Thailand. This group is comprised of community leaders, and were asked to advise on study design, process, and outcomes of interest, and subsequently approved the study (TCAB-9/2/2015).
Results
From 2004 to 2016, 5611 women met IG-21 inclusion criteria, apart from height and formal education requirements.31 A total of 4340 (77.3%) newborns, roughly three in four, were classified as AGA (figure 1). The AGA analysis included 3180 (73.3%) refugee and 1160 (26.7%) migrant women (table 1). The median (IQR) gestational age in term AGA newborns was 39.2 (38.5–39.6) weeks.
Maternal characteristics and birth outcomes, by BMI category (n=4340)
SGA and LGA
Of the newborns excluded (1271, 22.7%), 981 (17.5%) were SGA and 290 (5.17%) were LGA by either IG-21 or GROW standards; 442 (7.88%) were identified as SGA and 111 (1.98) as LGA by both standards. Prevalence of SGA was lower by GROW standards at 8.2% compared with IG-21 standards at 17.2% and LGA was low overall, but higher by GROW standards at 4.8% than by IG-21 at 2.4% (online supplemental table 1).
Supplemental material
Maternal stature and BMI categories
The proportion of underweight women was higher than overweight and obese combined (632 (14.6%) vs 469 (10.8%)) (table 1). Mean height (SD) for women with AGA term newborns was 151.5 cm (5.13) (table 1). Each centimetre of height was associated with an 11 g increase in newborn weight (95% CI 9.61, 12.7). A majority of this cohort, 58.5% (2539), would have been excluded by the IG-21 height criteria set at <153 cm.31
GWG by BMI and maternal stature
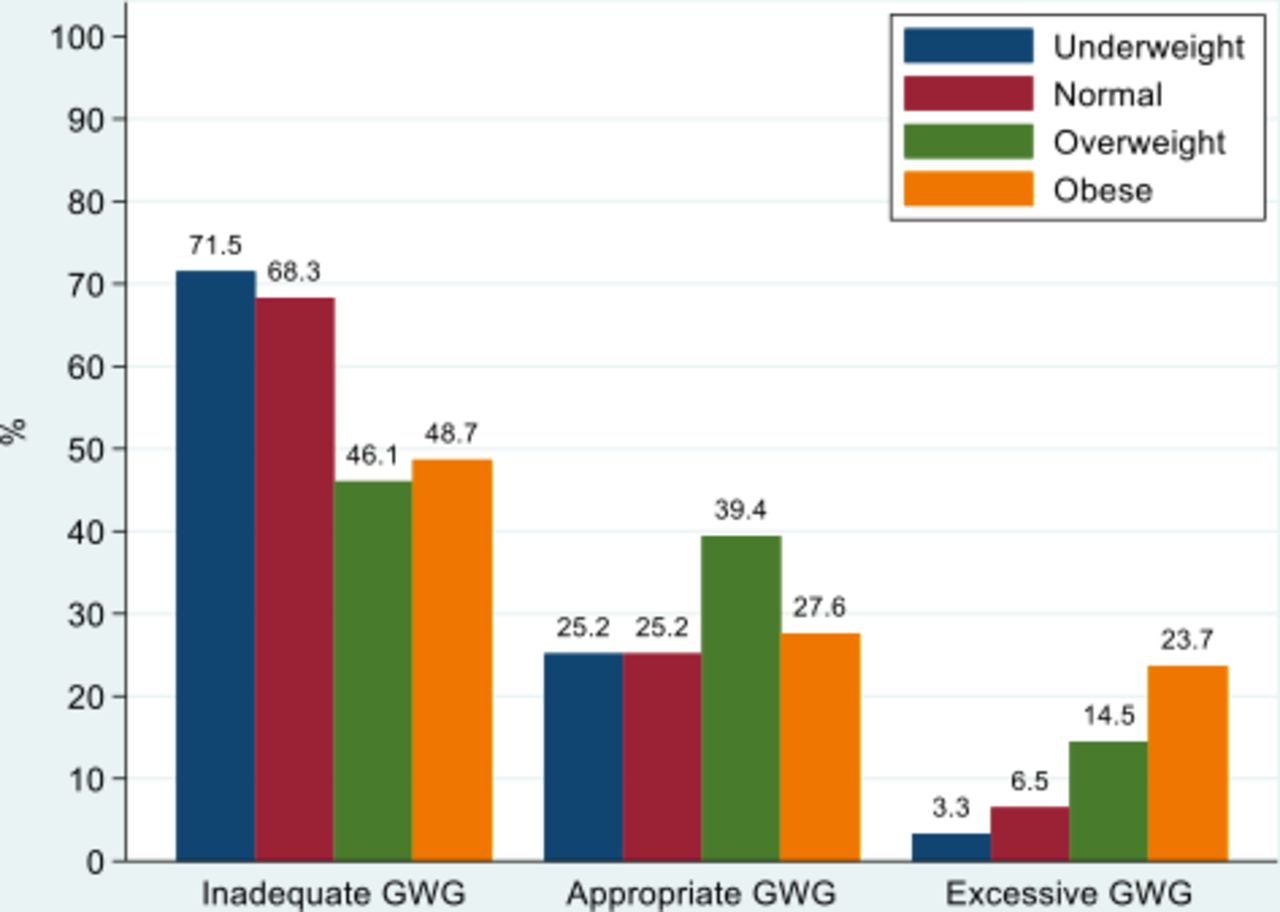
Mean GWG (SD) decreased as BMI increased: underweight 10.9 kg (3.3), normal 9.9 kg (3.7), overweight 7.6 kg (4.1) and obese 5.9 kg (4.8) (table 1, p<0.001 for trend). Overall, across all BMI categories, only one in four women (1150/4340, 26.5%) had GWG within the range recommended by NAM. The proportion of inadequate, excessive and appropriate GWG for each BMI category demonstrated that approximately 70% of under- and normal weight women had inadequate GWG by NAM (figure 2). Nearly two-thirds of overweight and three-fourths of obese women did not meet the NAM-recommended GWG, and one in four obese women had excessive GWG.

Among those birthing appropriate for gestational age newborns (n=4340), the proportion of participants with inadequate, appropriate or excessive gestational weight gain (GWG) by NAM GWG guidelines for each BMI category. BMI, body mass index; NAM, National Academy of Medicine.
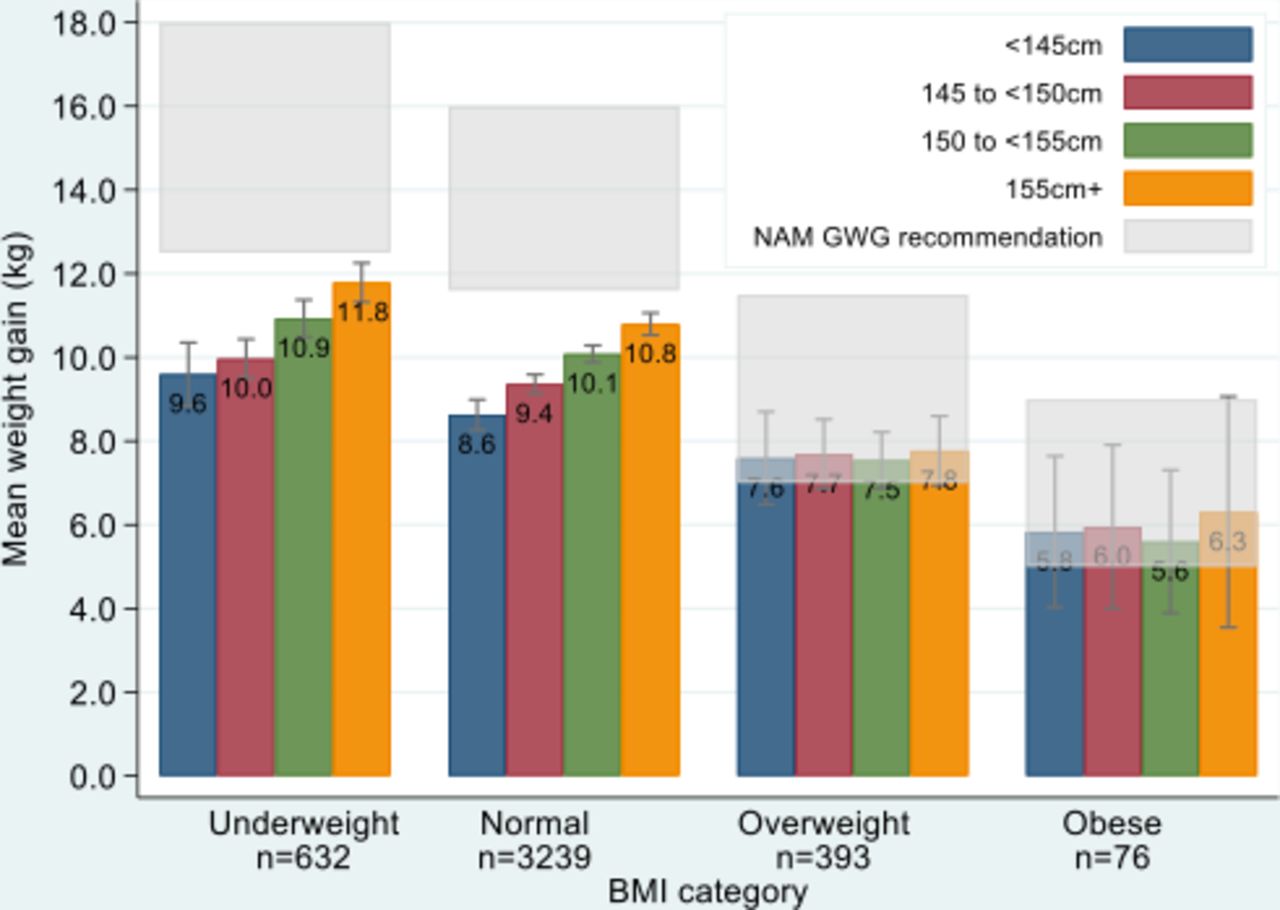
Among underweight and normal BMI women, mean GWG was lower than the NAM GWG recommendations for any height (figure 3). For these women, lower height had a significantly lower mean GWG compared with women who were taller (p<0.001 for both BMI categories, figure 3). The weight difference between women <145 cm and women ≥155 cm was 2.2 kg for both underweight (9.6 and 11.8 kg) and normal (8.6 and 10.8 kg) BMI categories (figure 3). The overweight and obese BMI categories had smaller sample sizes and mean GWG did not differ by height (p=1.0 and p=0.85, respectively), and fell within the lower range of recommendations provided by the NAM GWG guidelines.
{kind=link}
{kind=link}
{kind=link}
Mean gestational weight gain (95% CI) stratified by height and BMI category (n=4340). Grey boxes indicate NAM GWG recommendation ranges (12.5–18.0 kg, 11.5–16.0 kg, 7.0–11.5 kg, and 5.0–9.0 kg for underweight, normal, overweight and obese women, respectively). BMI, body mass index; NAM, National Academy of Medicine; GWG, gestational weight gain.
Discussion
This study sought to understand how maternal stature, BMI and GWG relate to each other among AGA newborns in an Asian population where short maternal stature is the norm. The study population is among the shortest maternal stature cohorts in the literature reporting on BMI, GWG and newborn birth weight for gestational age in term infants34 35 with three in four women birthing AGA newborns by international standards. These same standards would consider more than half of the women who birthed AGA newborns unhealthy: nearly two-thirds of the women would be excluded as ‘too short’ by IG-21 and two-thirds have suboptimal GWG according to NAM recommendations.
The most important finding for underweight and normal BMI women—90% of those birthing AGA newborns—was the significantly lower mean GWG in women of short stature who failed to reach NAM GWG recommendations. These women give credence to the suggestion that the ‘special populations’ alluded to in the NAM recommendations do indeed exist, and that maternal height should be considered with pre-pregnancy BMI. The NAM guidelines go on to recommend that women <157 cm gain at the lower end of the GWG recommendations according to their BMI,2 and, as expected, this study finds that GWG decreases with decreasing height.
Although significant for underweight and normal BMI women, a trend of increasing maternal stature with increasing GWG was not observed for overweight and obese women. Either there is no trend36 37 or study limitations may prevent a trend from emerging. Limitations may include: (1) more overweight/obese women are required to demonstrate a pattern as they have a 30%–40% lower mean overall weight gain compared with underweight and normal weight women; (2) misclassification of women according to international BMI categories instead of those proposed by WHO for Asian populations7 and (3) newborns who would be effectively LGA if using local standards may be misclassified as AGA using international standards.38 39
Other study limitations include its retrospective design, and we must agree with NAM that prospective studies in populations with short maternal stature are needed.2 For the purpose of this analysis GWG was was not linked to adverse pregnancy outcomes, which were excluded. Further analysis including the relationship between GWG and adverse pregnancy outcomes is planned. Some study strengths, however, include a well-defined cohort of marginalised populations, summarising information important for limited resource settings. Among included and excluded women, trends for maternal characteristics and newborn birthweights were consistent across BMI categories as reported in other populations,40 indicating robust data. Additional strengths are the utilisation of inclusion/exclusion criteria from the published literature to allow for comparison with other ‘healthy’ women, and use of consistent and accurate methods for measuring variables and outcomes.
There is a dearth of literature on GWG recommendations for women of very short stature who are overweight and obese such as those found in this population. Should these women meet the median or upper ranges NAM recommends, it is cause for alarm as the risk of adverse pregnancy outcomes is likely to be increased.39 The nutrition transition is accelerating in limited resource settings19 41 42 and, as shown in this population, it is critical that appropriate recommendations be developed that optimise outcomes across all BMI categories. International standards should take into consideration WHO Asian BMI categories in order to accurately stratify risk of non-communicable diseases in pregnancy for Asian women. In addition to prospective studies, data pooling across settings in Asia or meta-analyses can help untangle the problem of misclassification and clarify appropriate GWG recommendations that take into account maternal stature as well as BMI.
Acknowledgments
We would like to thank the pregnant women who attended ANC early in pregnancy and birthed at SMRU. This work would not be possible without the tireless effort of the SMRU ANC and midwifery staff, mostly from the very same communities as many of the women in this study. We would like to thank Dr Nicola Solomon for her work on cleaning BMI data and Drs Emma Plugge and Kremlin Wickramasinghe for their support in acquiring funding through the John Fell Fund.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Sanni Yaya
SJL and AHH contributed equally.
Contributors SJL: Conceptualisation, data curation, formal analysis, investigation, methodology, software, validation, visualisation, roles/writing—original draft, writing—review and editing. AHH: conceptualisation, formal analysis, funding acquisition, investigation, methodology, visualisation, roles/writing—original draft, writing—review and editing. AMM: data curation, project administration, validation, writing—review and editing. MEG: data curation, project administration, validation, writing—review and editing. NWT: data curation, project administration, validation, writing—review and editing. LLW: data curation, project administration, validation, writing—review and editing. MW: data curation, project administration, validation, writing—review and editing. EW: data curation, Project administration, validation, writing—review and editing. MN: data curation, project administration, validation, writing—review and editing. PC: funding acquisition, project administration, writing—review and editing. FHN: funding acquisition, resources, writing—review and editing. VIC: conceptualisation, formal analysis, investigation, methodology, validation, visualisation, roles/writing—original draft, writing—review and& editing. RM: conceptualisation, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, visualisation, roles/writing—original draft, writing— review and editing.
Funding This study was funded as part of the Wellcome-Trust Major Overseas Programme in Southeast Asia (grant number: 106698/Z/14/Z). Supplementary funds were also provided by the John Fell Fund, UK (project code: B9D00030).
Disclaimer The funders had no role in the collection, analysis or interpretation of the data, the writing of the article, or in submission of the paper for publication. The views expressed in the paper are those of the authors and do not represent the positions of their respective institutions or that of the funding agencies.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval for this study was given by the Oxford Tropical Research Ethics Committee (OXTREC 28–09) in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on request. The data used to support the findings of this study may be released upon application to the Data Access Committee at Mahidol-Oxford Tropical Medicine Research Unit (MORU), who can be contacted at: https://www.tropmedres.ac/units/moru-bangkok/bioethics-engagement/data-sharing.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.